Parents as Partners in the NICU

The latest featured article in the current issue of ANS is by Amy L. D’Agata, PhD, MS, RN and Jacqueline M. McGrath, PhD, RN, FNAP, FAAN, titled “A Framework of Complex Adaptive Systems Parents As Partners in the Neonatal Intensive Care Unit.” The article is available for download at no cost while it is featured. Dr. D’Agata sent this message for ANS readers, portraying the important interplay of her clinical experience and academic science to create new insights and new practices to improve care:

Amy D’Agata
I am honored to have my paper A Framework of Complex Adaptive Systems: Parents as Partners in the Neonatal Intensive Care Unit featured as an editor pick in Advances in Nursing Science. This paper highlights complexities within the NICU, particularly around relationships and environments of care that may contribute to infant neurodevelopmental outcomes. It is hoped that by acknowledging challenging factors of interpersonal communication, individual differences in practice and acute care environments, we may begin to redesign the current NICU model of care into a model that better promotes neurodevelopment. Importantly, reframing how we think about parents and their participation in the care of their infant.
As a novice neonatal intensive care nurse, I loved the excitement the NICU provided, both from a technical and interpersonal perspective. Through advances in technology and medicine, precious newborn lives were saved and family dreams were realized. Supporting families as they went through a sea of emotions, learned who their baby was as a person and became a strong advocate for their baby. I always loved working with families and helping them through this process, all while I was caring for their baby. This is how we practice in the NICU, right? By and large, nurses and physicians care for patients while families stand by and watch, right? This is what has to happen in order to save lives, right? We know best, right? This is basically how we have always been trained, but now I wonder if there isn’t a different and better way.

Jacqueline McGrath
After 14 years of professional nursing practice, I entered doctoral studies. Early in the program I felt as though I was floundering because my research interests were all over the map. I knew my population of interest would be NICU infants, but I wanted to fix lots of different issues. Most of which were medical issues. When potential ideas around developmental care were suggested by my advisor (and co-author) I quickly pooh-poohed them. Developmental care was a fundamental component of NICU care, but not in my wheelhouse to study.
One day my doctoral advisor shared an article she had co-authored, Epigenetics and Family-Centered Developmental Care for the Preterm Infant.1 At the time I knew nothing about epigenetics so I was immediately curious. After reading this paper I literally experienced a professional paradigm shift. Swiftly brought into focus was the idea that all of our daily experiences impact us. While this may not seem like a game-changing statement, the fact that seemingly insignificant experiences may trigger molecular changes was something I never considered. This certainly wasn’t something I considered for our patients.
I have always passionately believed that the work we do in the NICU is important to an infant’s future, but as a nurse, I had practiced with the thought of meeting the necessary medical needs so that infants may one day leave the NICU with their family. I didn’t intentionally practice with the idea that everything I did in the NICU, every single day, may leave a permanent molecular mark or imprint that may shape who that person becomes. If I had understood the potential magnitude of my influence, I would have most certainly practiced differently early in my career.
Back to doctoral studies, following lots and lots of reading, my research program began to take shape. I read volumes about early life experience, epigenetics, genetics, molecular experiences that ‘get under our skin’ and neurodevelopment. During my academic studies I also continued practicing as a staff nurse in the NICU. This was a time in which I felt a lot of turmoil as a caregiver, because of what I was learning academically and what I was observing and taking part in clinically, sometimes I felt such internal conflict. To get through I need to reconcile that what I was learning from basic science was ahead of where we were clinically.
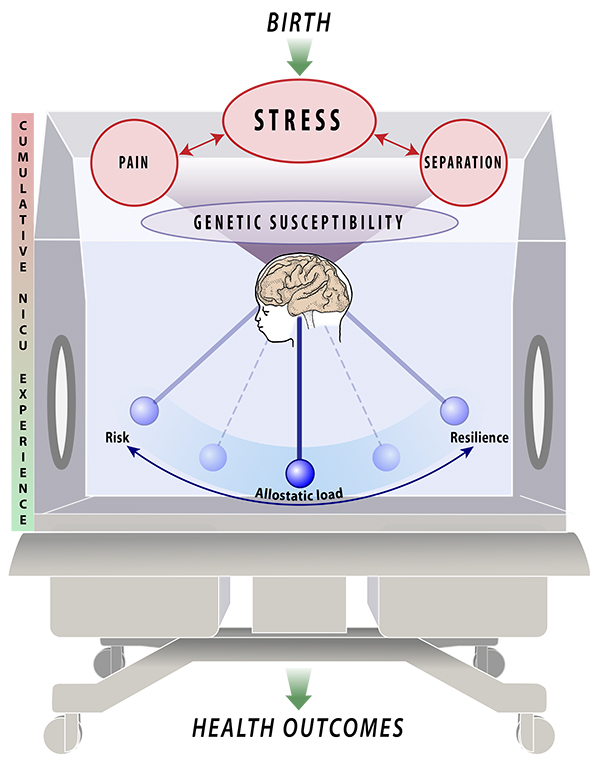
As a conceptual model and framework of the NICU infant experience, Infant Medical Trauma in the NICU, broadly reflects the adverse exposures that occur within the NICU doors and how they may contribute to long-term outcomes (see figure below). Designing this model was the foundational to my dissertation work for exploring the relationships between NICU stress, genotype of stress associated gene FKBP5 and neurodevelopmental outcomes. The goal of my dissertation study was to understand if some infants may be genetically more vulnerable to stress experiences in the NICU.
Understanding that some infants may be predisposed to stress sensitivity, and the dynamics of the NICU, parents may be ideally positioned for the role of co-caregiver. Given the typical parent’s desire to learn anything that helps their infant, their sensitivity to their infant’s needs and awareness of the role they must fulfill once they leave the NICU, why do we place parents on the sideline while we care for their infant? Are parents incapable of learning how to assess their infant or perform caregiving tasks beyond diaper changes, temperature measurement and feeding? We expect them to be fully capable once we indicate discharge is eminent, why not earlier in the process?
If we are to improve neurodevelopmental outcomes in the NICU, we may need to critically assess how we practice and consider alternative models. As care providers, our goal is to save lives and promote health. While not intentionally inflicted, there are adverse experiences that result from that goal. Parents are the constants in their infant’s life and the people who will care for their infant beyond the NICU. In light of this we must begin to see parents as partners in every step of the NICU, including in the provision of care.
- Samra, H., McGrath, J. M., Wehbe, M., & Clapper, J. (2012). Epigenetics and family centered developmental care of the preterm infant. Advances in Neonatal Care, 12(5s), s2-s9





thanks for interesting article – i was drawn by the line, “When parental care is replaced
by nursing care, a formidable nurse-patient relationship is established between the nurse and the infant” (p. 248). It is this contested space that it seems likely we (healthcare professionals) have some learning to do. Lupton & Fenwick (2001) perceptively highlighted this dynamic from their research with mothers in nicu/scbu; mothers felt like they had to wrest control back from nurses in their drive to complete their identity as mothers. Interestingly (as their focus was children with chronic illness rather than neonates), Dickinson, Smythe & Spence (2006) also note the complex web of relationships that families have to navigate to ensure appropriate care for their children. Your article will hopefully serve as a further cause for reflection for all of those of us who work with infants, children, and families.
Thank you for your comment. I agree with your statement that we have some learning to do. I do not believe we enter into practice with such an intention, to create boundaries, however I am becoming of the belief that there is a care provider acculturation. Many of us enter into practice and learn from those who become our mentors, and in that process adopt beliefs/norms that perpetuate certain practices. I think reflection is a great place to begin to rethink “how” we practice and what our beliefs are about ourselves as providers, as well as patients and families.
Thank you Amy. I certainly agree that understanding how to do this better is more complex than pathologising colleagues; that is, suggesting that the problem is simply ‘the nurses’, ‘the doctors’, etc. (and clearly your work did not oversimplify in that way :)) And yet there are colleagues who (whether consciously or unconsciously) enjoy the benefits of ‘power-over-other’ that they have by virtue of their role. I wonder whether this is where notions of post-structural contested power and approaches like actor network theory are helpful in exposing the interplay of personal-institutional-socio-cultural-economic factors? …and yet, at the heart of these discussions are human beings made vulnerable by circumstances and context. i hope we (as a collective profession) never lose sight of that. in my research with families (and children) i cannot escape the sense that partnership is never going to happen until each is (somewhat) known to the other – nurse and family.