In our current featured article titled “Veteran Competencies for Undergraduate Nursing Education,” authors Jacqueline A. Moss, PhD, RN, FAAN; Randy L. Moore, DNP, RN and Cynthia S. Selleck, PhD, RN, FAAN present the results of their project to address veteran health concerns that arise from their military service . The competencies they identified are: Military and Veteran Culture, Post Traumatic Stress Disorder, Amputation and Assistive Devices, Environmental/Chemical Exposures, Substance Use Disorder, Military Sexual Trauma, Traumatic Brain Injury, Suicide, Homelessness, and Serious Illness Especially at the End of Life. The article is available for free download while it is featured on the ANS web site!
Dr. Moss has provided a narrated slide show that explains the background of their project:
The current ANS featured article is titled “Screening for Obstructive Sleep Apnea in Veterans Seeking Treatment of Posttraumatic Stress Disorder,” authored by Lauren Forbus, BSN, RN and Ursula A. Kelly, PhD, ANP-BC, PMHNP-BC. Their article is available for free download while it is featured on the ANS website. Ms. Forbus shared this information about their work with veterans:
Our team began to take a look at obstructive sleep apnea (OSA) among veterans with posttraumatic stress disorder as a result of some unexpected findings in another project, Project Stress Less. Project stress less was developed to establish the feasibility of conducting a trauma-sensitive yoga intervention for women
Lauren Forbus
veterans with posttraumatic stress disorder (PTSD) who experienced Military Sexual Trauma (MST). Because sleep was a primary outcome of this study, OSA was initially an exclusion criterion. We assessed for presence of OSA through medical chart review and self-report during phone screening; and we assessed for risk for OSA using a questionnaire in our phone screening process. The unexpected finding in the screening process for this study was that 14.6% of those screened had been diagnosed with OSA and 63.2% were at high risk for OSA – both numbers that are greater than in the general population.
As we moved forward with Project Stress Less, we simultaneously began to think about implementing a larger OSA risk screening study into an outpatient VA PTSD clinic to get a bigger snapshot of what this risk for OSA looks like in the Veteran population. The idea was eventually implemented as the study described in our published article. What we found was consistent with our initial findings in Project Stress Less – a great majority of veterans were screening at high risk for OSA, however, only a small portion of them had documentation of a formal evaluation for OSA in their medical records.
These findings were significant enough that our research team proposed and is in the process of implementing a clinical practice improvement in collaboration with our VA colleagues in the PTSD clinic. The common goal is to develop screening, referral and follow up processes for Veterans who screen at high risk for OSA. Because of this supportive relationship with our VA colleagues, we have had the unique opportunity to quickly turn our research findings into meaningful practice change. So far we have inserted an OSA screening tool into the clinic’s intake packet, which is currently used for clinical purposes at intake as well as for program evaluation. We are also working on developing a follow up plan for those who screen at high risk. As we move forward with this practice change in the short term, we are keeping our eye on the long-term goal of conducting further research. Our hope is that we can gain new insights to help alleviate some of the sleep complaints that often times plague our Veterans with PTSD.
Share your comments here to engage in discussion about these important issues!
In our current ANS featured article, author Susan W. Durham, PhD reports her qualitative study of communication challenges experienced by service members in staying connected with their families. Dr Durham shared this background information about her work for ANS readers:
Coming from an early career in the US Army Nurse Corps and as a parent of an Infantry officer who was deployed to both Iraq and Afghanistan four times over the course of seven years, I was inspired to study the experiences of deployed service members in their attempt to stay connected to their families and loved ones while deployed in a combat environment. Doing these interviews and listening to the stories has been one of the greatest privileges of my life. Most of the
qualitative studies that looked at communication issues and deployment studied the experiences of family members and the service members’ voices were not being heard.
The benefit of content analysis, a form of qualitative research, doesn’t generally result in hard data or a bar graph. Some scholars even have difficulty understanding the value of this type of research and may ask, “Where do interviews and observations like these get us?” The short answer is that qualitative data provides context and meaning.
These interviews not only tell unique stories about individual service members’ experiences but also offer a collective understanding of common communication challenges for deployed individuals. Hearing and analyzing their stories and combining the results into a combined narrative provided multiple perspectives that no single participant could have related in totality. The interviews also accomplished what survey questions could not because every participant was able to express his or her personal, detailed experiences and observations of the phenomenon being studied. The description of the participants’ experiences enables the reader to understand the service members’ perspectives, perceptions, and reactions known only to them. Also, the results offered a collective viewpoint that ultimately will provide quantitative researchers with variables, issues, and hypotheses for future inquiry about communication issues experienced during deployment to a combat environment.
You can download a copy of this article at no cost while it is featured on the ANS web site – I urge you to do so now, and then return here to join me in expressing appreciation for the insights that Dr. Durham’s study provides.
Our current featured article addresses the application of nursing theory in practice, demonstrating how Kolcaba’s comfort theory provides an holistic approach for identifying needs, creating interventions to meet those needs, and for evaluating the effects of those interventions. The article is titled “Comfort Theory: Unraveling the Complexities of Veterans Health Care Needs” by Lina Daou Boudiab, MSN, RN and Katharine Kolcaba, PhD, RN. I invite you to download this article while it is featured on the ANS website, and after reading it, return here to enter into discussion of these important ideas.
Author Lina Daou Boudiab provided this message about her work for ANS blog readers:
Lina Daou Boudiab
A holistic approach to patient care has always been a preoccupation of mine since my early days in nursing. I have always been interested in interventions that embraced the art of nursing and extended beyond the physical to address patients’ needs effectively. Kolcaba’s Comfort theory highlights the holistic nature of our experience of health, in terms that make sense to patients and staff alike. It is simple, yet quite comprehensive and highly applicable. It acknowledges the various contexts that play into a person’s experience of comfort and health, valuing the psycho-spiritual, sociocultural, and environmental contexts on an equal footing with the physical.
Often when I discuss Comfort Theory with patients with chronic pain, explaining the difference between comfort and the mere absence of pain and why we would like to focus on comfort, there seem to be a sense of relief and empowerment as they say, “I never thought about it that way.” People seem to be stuck within the constraints of their comfort needs or symptoms, which tend to permeate every level of their being. Chronic pain impacts every context of a person’s comfort, which in turn accentuates the experience of pain. Anxiety and feelings of powerlessness similarly impact the person’s social interactions and heighten their experience of physical symptoms, among others. As I discuss with patients the contexts (physical, psycho-spiritual, sociocultural, and environmental) and aspects (relief, ease, and transcendence) of comfort, I believe there is a sense of hope and empowerment that blossoms, baring the possibility of comfort in their future. They seem to retrieve a sense of self beyond a physical entity with perceived limitations. Comfort Theory empowers staff and patients to invest in practices that would promote comfort in any of the discussed contexts to maintain a state of ease and encourage transcendence into a comfortable, highly functional state of being or, in case of palliative or hospice care, a peaceful death.
Furthermore, Comfort Theory allows us to measure the effectiveness of various comfort interventions, such as body-mind-spirit modalities, comfort rounding, active listening and presencing, among others. Incorporating a verbal rating scale (0-10) of comfort in documentation notes, in addition to that of pain and/or any other symptom, adds to the richness of patient assessment and outcome evaluation of particular interventions.
In our Healing Touch Comfort Clinic, few patients with chronic pain have expressed a change in the quality of their pain (for example from sharp to dull) after receiving healing touch, but still rated their pain at the same level as before the intervention. Nevertheless, they stated that they felt more comfortable and rated their comfort level higher than baseline. Throughout my nursing career, I have taken care of patients who rated their pain as moderate (between 4 and 7 on a 0-10 scale), yet felt it was still acceptable. They preferred the experience the pain over prescribed pain medications and their potential side effects and embraced non-pharmacological interventions to transcend it. I do believe that monitoring pain levels as the sole measure of effective pain management and overall patient comfort is inadequate and does not reflect the holistic nature of comfort nor patients’ individuality and personal preferences. Comfort Theory provides a framework for practice and tools to help us move towards a more effective and inspiring patient-centered model of care, focusing on positive outcomes of enhancing our patients’ comfort and their overall sense of wellbeing.
Disclaimer: The contents of this blog do not represent the views of the U.S. Department of Veterans Affairs or the United States Government.
Our current featured article is titled “Nurse Middle Managers’ Dispositions of Habitus: A Bourdieusian Analysis of Supporting Role Behaviors in Dutch and American Hospitals” by P. C. B. Lalleman, MA; G. A. C. Smid, PhD; M. D. Lagerwey, PhD; L. Oldenhof, PhD and M. J. Schuurmans, PhD. While it is featured, you can access this article at no charge on the ANS website, and welcome your comments here! Pieterbass Lalleman has prepared this video, followed by a blog message about this work:
The current featured article in ANS focuses on supporting roles of nurse middle managers. The paper is part of a larger Dutch study on nurse middle managers daily work. The main goal is to better understand the role of nurse middle managers in hospitals and their leadership. We wondered: What gives these nurse managers authority in their daily
work? Most literature on nurse managers advocate American nurse managers work within Magnet hospitals as the best practice model.
The study has been initiated by the Dutch HU University of Applied Sciences and the Dutch Nurses Association. We decided to investigate practices of nurse middle managers in Magnet, Magnet-related and non-Magnet hospitals in both the Netherlands and the United states. Our grant proposal has been awarded $300.000. This allowed us to have a close look at the work of nurse managers in both the Netherlands and the United States This funding made it possible to conduct research and shadow nurse managers in New York and Michigan for one year.
Based on this ethnographic work (560 hours shadowing), we made an interpretation of the work of nurse middle managers using Bourdieu’s tools of dispositions and habitus (or second nature), field and capital. In this ANS article we describe first describe some essential findings: the eight dispositions of habitus of nurse middle managers. A caring, clinical and scientific disposition seemed vital. In the next part we describe how a different configuration of dispositions of habitus of nurse middle managers influenced their authority in each of the four participating hospitals. In forthcoming articles, we will analyze how these configurations influence the emergence of nurse middle manager’s leadership.
In this blog we zoom in on two aspects of our research that were more on the background: 1) living and doing research in the U.S. and 2) the importance of doing research together.
Big Friendly Giant
I used to work as a nurse and manager in a hospital, and now I work as a lecturer and researcher in an University of Applied Sciences in The Netherlands. We choose to move with my family to the U.S. for one year and take our time to understand living and working in the U.S. from a Dutch perspective (and not fly alone to the U.S. for 4-5 times and conduct the shadowing in slots of 2-3 weeks). This was a lucky choice. Doing ethnography demands a deep and robust understanding of the world you are investigating. Living in New York, walking my two youngest daughters to PS 8, the Robert Fulton School in the morning, followed by a bike trip across the Brooklyn Bridge to drop-off my eldest daughter at the Lower Manhattan Community Middle School at 26 Broadway , helped me in understanding and comprehending what I saw during my days shadowing the nurse managers. Although every hospital looks alike on first sight, especially during quick visits or tours, deeper insight is created by ‘hanging around’ for a longer time. Both shadowing as a research method for ethnography and moving to the U.S. were crucial for describing the habitus or second nature of these nurse managers. As a shadower I literally have been in the shadow of these, mostly women, that I followed during work. I am 6 feet and 5 inches tall a rather large shadow for these nurse managers. On a particular day a staff nurse of the hospital in Queens came to me smiling and said: ‘there you have the Big Friendly Giant again’. This reference to Roald Dahl expressed exactly how I felt in the strange new world that I thought I knew so well (both the hospital world and the U.S from the hundreds of articles, movies and TV shows). These kinds of encounters and also the experiences of my children and my partner helped me with making sense of the work of nurse managers in their hospitals and reflect on my own presence and interpretations. My work would not have been possible if I just have been visiting for a couple of weeks.
Reflection on wheels: the importance of ‘member check’ and collaborative research
This research project was an ethnography inspired by action research. The grant money gave us the opportunity to organize member check sessions with the nurse managers to report on the preliminary findings and discuss the meaning of these. The first session was organized in The Netherlands after we finished shadowing at the two Dutch sites. A very interesting finding of that session was that the nurse managers from the two sites requested to shadow each other. Their main motivation was that being shadowed helped them with the recognition of habitus as a second nature, their routine behavioral repertoire became exposed during shadowing. Shadowing someone else who was doing the same job enhanced their understanding of their daily work and habitus. The objects of this study, the nurse managers, became researchers (or subjects) of their own work. This movement became even more visible when the eight Dutch nurse managers (and my Dutch PhD supervisors) joined me in the U.S. for a one-week research trip to the two American hospitals. The 6-day trip started on a Sunday at NYU’s Institute of Public Knowledge were I met these Dutch managers and discussed the program with them. On Monday and Tuesday, we would visit the partner university and the hospital I shadowed in New York. On Wednesday we had a 733 miles’ bus trip from New York to Western Michigan. On Thursday and Friday, we visited the hospital and university in the Mid-West.
For me, as a researcher it was great to finally share all my observations with the nurse managers of the Netherlands, show them the U.S. system in full color. It also, helped me reflect on my findings and putting them in perspective. After two full days of New York, (Live in New York City once, but leave before it makes you hard) the 10 hour coach ride was one of the greatest reflective experiences I had during this PhD project. The drive through the state of New York, Pennsylvania, Ohio, Indiana and Michigan was superb. It gave us a change to reflect on all the impressions of New York and prepared us ready for the friendly Mid-West. I had the chance to talk the Dutch managers, interview them, record their experiences and illustrations. They did not only talk about the U.S., they also talked about home, how nursing and nurse management is organized in their own institutions. Travels like these can be very inspirational and valuable. Travelling enhances reflection. It creates new insights and helps both researcher and participants in making sense of the phenomenon under investigation.
In sum, PhD research tracks like these are like journeys in which both researcher and participants of the study collaborate to find the answers to complex challenges. To accomplish this the researcher, have to be close to the subject, live and work with them to fully grasp and comprehend the essence of what is seen. Both shadowing, member checking sessions and an international research trip contribute to these outcomes.
I would like to thank all the nurse managers and my supervisors for realizing this first publication on nurse middle managers daily work.
The current featured ANS article provides an example of an approach to knowledge development that delves deeply into the narrative of the lived experience of a single person. The article is titled “Being the Mother of an Adolescent Suffering From a Spinal Cord Injury: Possibilities of a Personal Narrative in Phenomenology.” The author, Sanne Angel, PhD, RN, is from Aarhus University in Denmark. Here is her message reflecting on this method and its potential for developing nursing knowledge:
From a decade of studying life after spinal cord injury I draw attention to the craft of the single story. Its force in relation to develop a caring attitude is unsurpassed. Maybe this should be used more, both in relation to the professionals in charge for the patient and the
Sanne Angel
politician responsible for the needed resources. Thus in its own right, the individual analysis invites us to lend such an ear to the possibility of how others might experience this phenomenon, here “Being the mother of an adolescent suffering from a spinal cord injury”. And that is the real thrust of the study here.
Further as a methodological contribution, I am suggesting that the move from one person’s experience to others’ is itself supported by the implicit “eidos” of the single. From the analysis of the single story it is possible to extract what could be true for other people in similar situations. This move from one to another lived context requires an act that is not unlike Husserl’s own move from one case to his imagined variations.
However, performing an imaginary variation is what is done also when more than one single case, and may take a very talented researcher (which I do not claim to be). This calls for external validation judging whether this is done successfully, and I welcome you readers to engage therein.
Please visit the ANS site while this article is featured and available for free download! We welcome your comments and ideas in response to this thought-provoking article!
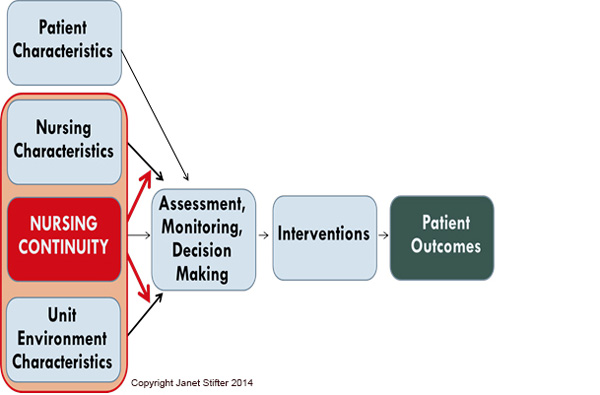
The current featured article in ANS focuses on using health information technology to improve care for people who suffer hospital-acquired pressure ulcers. The article is titled “Proposing a New Conceptual Model and an Exemplar Measure Using Health Information Technology to Examine the Impact of Relational Nurse Continuity on Hospital-Acquired Pressure Ulcers” by Janet Stifter, PhD, RN; Yingwei Yao, PhD; Karen Dunn Lopez, PhD, MPH, RN; Ashfaq Khokhar, PhD; Diana J. Wilkie, PhD, RN, FAAN and Gail M. Keenan, PhD, RN, FAAN. Dr. Stifter shared this message about her work and additional information about the article:
The story of this manuscript began with my decision to go back to school to earn my PhD, 24 years after gaining my MSN and 30 years long years after gaining my BSN (my midlife “brain re-energizer” event). In 2011 I reached a career crossroads that led to a transition into graduate school as a full time PhD student at the University of Illinois in Chicago (UIC), College of Nursing.
Dr. Stifter
In my position immediately prior to entering the PhD program I was a Chief Nursing Officer (CNO) of a 300 bed community based teaching hospital who grappled daily with decisions around nurse staffing. Like many CNOs I was overseeing clinical areas operating under financial constraints and trying to meet or exceed a productivity metric at the 25% while maintaining high levels of quality, safety, and patient satisfaction. A significant source of frustration was the absence of real time, readily accessible, meaningful data to help me demonstrate to non-nursing executive leadership the possible association between our staffing decisions (floating; downsizing/ consolidating, and closing units; use of temporary and part-time personnel) and possible adverse patient outcomes.
At the same time, a second major imperative driving both the budget, manpower issues, and discussions around patient care outcomes was our uptake of a new electronic health record (EHR). I felt strongly that the answer to my data deficit was there in the new EHR, but how to access it? I wanted to work smarter and become more knowledgeable about engaging in this new world of EHR big data science. With the UIC doctoral program I recognized a clear synergy between my clinical issues, research interests, and the work of Dr. Gail Keenan and the HANDS (Hands On Automated Nursing Data System) team. Dr. Keenan’s HANDS database, an electronic nursing plan of care system, actualized my vision of using the EHR, with data being collected as part of routine nursing documentation, to begin examining the influence of nurse staffing on patient outcomes.
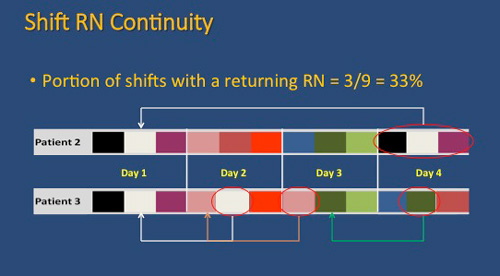
My specific focus on nurse continuity as a critical nurse staffing variable evolved out of a discussion with members of the HANDS team one day in our simulation lab at the university. Dr. Yingwei Yao, the statistician for the HANDS team, had created schematic diagrams using bands of color to visually depict the poor continuity of caregivers in sample admissions found in the HANDS database. A startling finding in these random examples was how few RN staff actually had the opportunity to care for the same patient within the same admission. What was also startling was that almost everyone around the table participating in the discussion could relate a similar story of having a family member, friend or themselves cared for with little to no continuity of nurse caregivers while hospitalized. Finally, a key driver to my study of nurse continuity was how little was published in the nurse staffing literature on this topic.
Despite the fact that it seems to be such a clearly held assumption by RNs that continuity in nurse staffing would lead to better outcomes, there is little data to substantiate this hypothesis, and in many institutions our staffing priorities are leading to anything but nurse continuity at the bedside. These early discussions and the lack of studies in the literature were the seeds to my PhD dissertation, an examination of the association of nurse staffing variables, including nurse continuity, on the development of hospital-acquired pressure ulcers, using HANDS as the data source to operationalize my study variables.
The genesis of this manuscript was the discovery during my literature review that some of the difficulties that arise from studying nurse continuity is due to the diverse definitions of the term and the absence of systematic methods for measuring the influence of continuity. I was also unable to locate a conceptual model that depicted continuity as I felt it operated – both as a direct influence on patient outcomes as well as a moderating influence on other nurse-staffing variables such as experience, education, and nurse-to-patient ratios. Thus, the purpose of this manuscript is to summarize the available research on nurse continuity and to present a framework and an innovative method for research regarding the influence of nurse continuity on patient outcomes.
Working with the HANDS team and this program of research has allowed me to blend 34 years of clinical experience with an academic inquiry around the issues of technology, nurse staffing, and patient outcomes. I have been exposed to the worlds of patient centered outcomes research, big data science, and data mining techniques through a research team that includes engineers, computer scientists, and nurses experts. I have also had the opportunity to create a conceptual model that moves nurse continuity into the mainstream of discussion around nursing staffing variables and patient outcomes. The next steps for this research program and the HANDS team includes a comparative analysis of indices used for measuring continuity and a replication study examining the influence of nurse continuity and other nurse-staffing variables on pain outcomes.
I hope you will enjoy this manuscript and look forward to your comments. Janet
I join Janet in inviting you to download this important article while it is available at no cost, read it, and return here for some good online conversation!
Our current featured article addresses one of the great concerns in health care today — evidence-based Intervention (EBI), or the adoption and implementation of practices that are supported by research evidence. The title of the article is “Synthesizing Marketing, Community Engagement, and Systems Science Approaches for Advancing Translational Research.” by Shawn M. Kneipp, PhD, RN, ANP-BC, APHN-BC, FAANP; Jennifer Leeman, DrPH, MDIV; Pamela McCall, BSN, RN, MPH; Kristen Hassmiller-Lich, PhD; Georgiy Bobashev, PhD; Todd A. Schwartz, DrPH; Robert Gilmore, BS; Scott Riggan, BA; and Benjamin Gil. This is a thought-provoking article that adds significantly to the ongoing discussion of the meaning of “evidence,” and the issues surrounding the links between and among research, theory and practice. Here is the abstract of the article:
The adoption and implementation of evidence-based interventions (EBIs) are the goals of translational research; however, potential end-users’ perceptions of an EBI value have contributed to low rates of adoption. In this article, we describe our application of emerging dissemination and implementation science theoretical perspectives, community engagement, and systems science principles to develop a novel EBI dissemination approach. Using consumer-driven, graphics-rich simulation, the approach demonstrates predicted implementation effects on health and employment outcomes for socioeconomically disadvantaged women at the local level and is designed to increase adoption interest of county program managers accountable for improving these outcomes in their communities.
I invite you to read this article and consider ways the ideas might advance our collective interest in strengthening the connections between evidence and practice. Visit the ANS web site today to download itt, and return here to add your comments and responses!
Even a casual scan of daily headlines makes evident widespread global suffering. In recent weeks distressing images have highlighted the desperate plight of refugees trying to escape violence in Syria, Afghanistan and Iraq. There is an urgent need to change global conditions of injustice, violence and environmental damage. Only when these underlying conditions are addressed will we be able to achieve a sustainable health for humanity. In recent years there have been numerous scientific reports linking social conditions such as violence and social injustice to health. This summer, agreement was reached on language for a draft United Nations (UN) agreement on the Sustainable Development Goals, a new agenda for human development through the year 2030. The document, Transforming our World: The 2030 Agenda for Sustainable Development, will be finalized and adopted at a special UN summit in September. https://sustainabledevelopment.un.org/post2015/transformingourworld
This visionary document makes clear the interdependence of multiple domains including health, peace, education and ecology. Nursing will be a critical force in achieving sustainable development over the next fifteen years. The article in the current issue of Advances in Nursing Science, “Transcendent Pluralism: A Middle-Range Theory of Nonviolent Social Transformation through Human and Ecological Dignity”, provides a framework for nurses to use in advancing nonviolent social transformation. Although it is written primarily from the context of societal issues I envision the theory as something nurses can use when working for institutional change within health care settings as well.
Working together we can truly transform the world and build a sustainable healthy global community.
You can access this article in the PAP (Published Ahead-of-Print) section of our web site! Please read it, and return here to share you ideas!
Nancy Murphy, NP, PhD is the author of our current featured article titled “Advancing the Interdisciplinary Collaborative Health Team Model: Applying Democratic Professionalism, Implementation Science, and Therapeutic Alliance to Enact Social Justice Practice.” In the article she examines three foundational pillars of social justice practice: democratic professionalism, implementation science, and therapeutic alliance to advance this practice. Dr. Murphy has provided this description of her work:
I can’t recall when I have not been thinking about interdisciplinary collaborative team work, its value, its challenges, and the ongoing effort to keep the patient in the center of care! As my early career coincided with the emergence of the HIV/AIDS epidemic, I was fortunate to be part of dynamic and
Dr. Nancy Murphy
creative interdisciplinary work, both in the hospital and the community setting. The early HIV models of care were immediately collaborative, as it was clear that one discipline alone could never provide all of what was needed. The “team” went beyond clinicians to include not only patients and families, but friends, communities, legal advocates, spiritual providers, and many other ‘partners in care.’
Decades later I am still at it, now hoping the application of democratic professionalism, implementation science and therapeutic alliance may advance and improve the Interdisciplinary Collaborative Health Team model. The ideas of task sharing, thoughtful and strategic implementation, and therapeutic alliance among and between colleagues, patients, families, communities, and systems are extremely timely, especially as the US ventures into reorganization of health care financing: Affordable Care Act, Accountable Care Organizations, Bundled Payments, etc. Burwell, the Secretary of HHS, has set forth a range of upcoming changes in reimbursement that are claimed to reward value over volume. The question is open as to whether these strategies are able to fulfill the social justice goal of both improving individual health outcomes and health disparities while simultaneously addressing larger health inequities (social, political, economic) that drive the negative social determinants of health.
I continue to rely on Audre Lorde’s advice and offer it here for others to consider, “Only within the interdependency of different strengths, acknowledged and equal, can the power to seek new ways of being in the world generate, as well as the courage and sustenance to act where there are no charters” (Sister Outsider, 1986, p. 111).
Visit the ANS web site now to download your copy of this thought-provoking article while it is featured! We welcome your comments and ideas!
The essential purposes of ANS are to advance the development of nursing knowledge and to promote the integration of nursing philosophies, theories and research with practice. We expect high scholarly merit and encourage innovative, cutting edge ideas that challenge prior assumptions and that present new, intellectually challenging perspectives. We seek works that speak to global sustainability and that take an intersectional approach, recognizing class, color, sexual and gender identity, and other dimensions of human experience related to health.
This journal is a member of, and subscribes to the principles of, the Committee on Publication Ethics (COPE) www.publicationethics.org
The ANS Blog provides a forum for discussion of issues raised in the articles published in Advances in Nursing Science. We welcome all authors and readers to post your comments and ideas on the blog! If you would like to be an author on this blog, let us know!
The journal Editor is Peggy L. Chinn, RN, PhD, FAAN. Dr Chinn founded the journal in 1978.




 nd Afghanistan four times over the course of seven years, I was inspired to study the experiences of deployed service members in their attempt to stay connected to their families and loved ones while deployed in a combat environment. Doing these interviews and listening to the stories has been one of the greatest privileges of my life. Most of the
nd Afghanistan four times over the course of seven years, I was inspired to study the experiences of deployed service members in their attempt to stay connected to their families and loved ones while deployed in a combat environment. Doing these interviews and listening to the stories has been one of the greatest privileges of my life. Most of the